We receive a number of emails from women looking into hairline lowering procedures due to having a high forehead. Dr. Shelly Kabaker of Oakland, California has become world renown for his excellent forehead lift procedure, which women with naturally high foreheads in particular can benefit from. We think women with this high hairline attribute would benefit from learning more about this procedure. The below describes procedures available for women with a high forehead interested in lowering their hairline. The article is long, but well worth the read.
To review a technique and to make quantitative analyses of the senior author’s 20-year experience with his preferred technique to correct the high female hairline.
Methods:
A retrospective review of 29 female patients with a high forehead who underwent the hairline-lowering procedure performed by the same surgeon (S.S.K.). We analyzed preoperative and postoperative standardized photographs by taking measurements from the medial and lateral canthi to the anterior hairline. Facial height, from the menton to the hairline, was also measured. We calculated mean values and then used a 2-tailed, paired to test to evaluate for statistical significance. Patients also underwent evaluation for satisfaction, complications, and aesthetic result. We reevaluated the measurements from the profile view and compared them with the original data.
Results:
The photographed midfrontal hairline position was vertically lowered on average 1.3 cm in patients who underwent a single-stage procedure (P.001). In retrospect, the analysis was flawed compared with clinical experience. Therefore, the profile views were evaluated, and the correlating true curvilinear advancement was an average of 2.1 cm. Three complications occurred,including 1 major effluvium, 1 minor effluvium, and 1 scar that required revision. Patient satisfaction was extremely high.
Conclusions:
Advancement of the female hairline and lowering a high forehead by incorporating an irregular trichophytic incision and a posterior scalp advancement flap is an effective and safe technique that has been used by the senior author for more than 2 decades. The average advancement was 2.1 cm in this study. The technique is immediately effective, well tolerated by patients, and associated with minimal complications. Although it is associated with a potentially visible incision, this technique can be used to make the scar virtually invisible. Arch Facial Plast Surg. 2009;11(2):84-90
Click here for a video demonstration of the female hairline lowering procedure
IN CLASSICAL AESTHETICS, THE FACE can be split into vertical thirds, a characteristic of well-balanced and attractively proportioned faces.1,2 The female hairline is variable in position. In the ideal situation, the hairline is 5 to 6 cm above the medial brows at the trichion, the point where the scalp slopes from a more horizontal to a more vertical position.3
In contrast, a number of women have high foreheads and thus, higher hairlines. The primary cause in most of these patients is heredity. These patients have a hairline that is usually stable after puberty without continued recession, and they have adequate hair density. However, these patients contend that their large high forehead and posteriorly displaced hairline make them look masculine, older than their respective years, and less attractive. 4 They are also unhappy because their high hairline limits their hair styling to bangs, which are used as camouflage.4 Depending on the hair texture and the exit angle of the hairs, bangs may not always be effective.
In addition, the number of iatrogenic high hairlines is increasing because of the growing popularity of endoscopic browlifts. 2,5 Because the forehead and scalp are moved posteriorly as a unit in an effort to raise the brows, the position of the anterior hairline is often significantly elevated. 6 Despite having a good brow position, these patients continue to have facial disharmony because of their disproportionately large foreheads and their disrupted aesthetic vertical thirds.4 It is our observation that, in many of these cases, the forehead skin stretches and the hairline is raised a greater distance than the brow is elevated.
Women with high hairlines of iatrogenic or hereditary causes may seek treatment. In this study, we review the senior author’s experience (S.S.K.) in addressing this situation. We present his current technique for correcting the high female hairline, and we evaluate its effectiveness and safety in treating these patients.
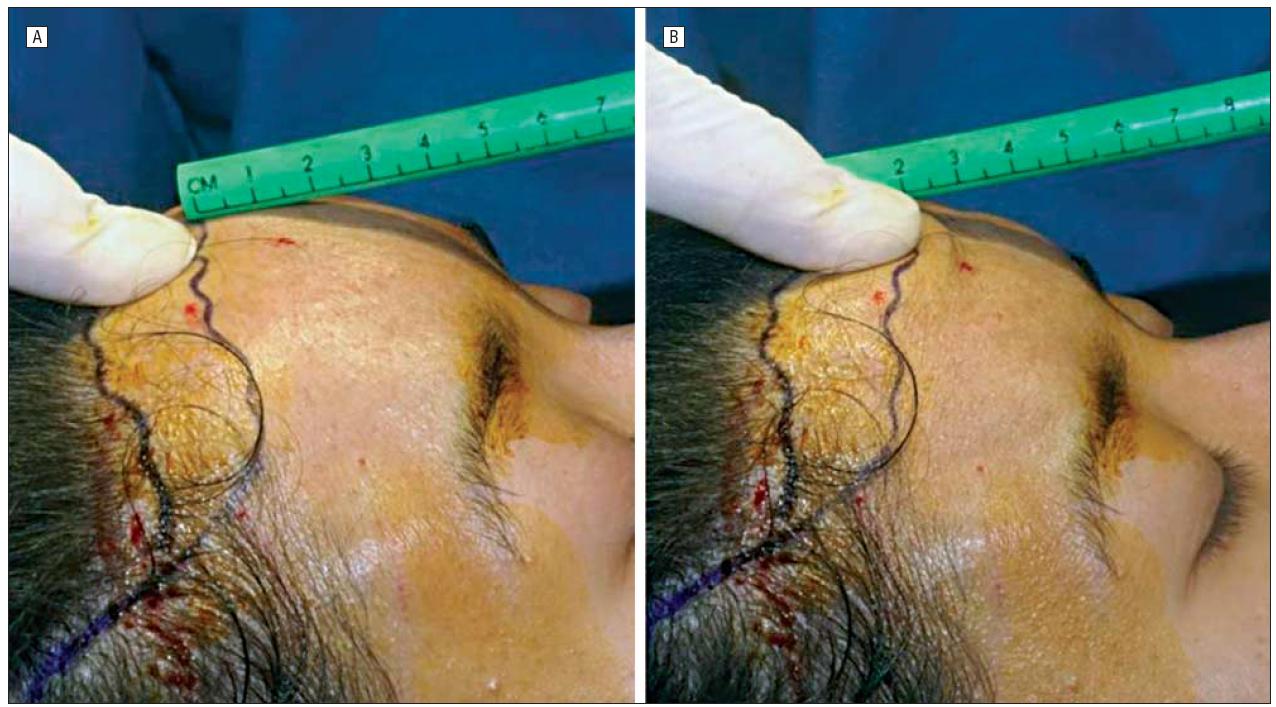
Figure 1. Preoperative evaluation for adequate scalp laxity. A, To determine adequate scalp flexibility, a point is chosen below the hairline and pushed as high as possible. his point of the fingertip is set to 0 at the hairline. B, The fingertip is then pushed as far downward as possible and a measurement is taken. Two centimeters of excursion typically allows for 2 cm of hairline advancement.
METHODS
We retrospectively analyzed 29 of 74 female patients with high foreheads from January 3, 2000, to November 2007 who underwent a 1-stage (no scalp expansion) hairline-lowering procedure in the senior author’s private practice (S.S.K.). Patients underwent preoperative evaluation with a history and physical examination, with specific evaluation of the hairline position for ongoing hair loss, scalp laxity, and a history of previous forehead or scalp procedures such as coronal or endoscopic brow-lift. Patients who had previous coronal brow-lifts or ongoing alopecia were not offered this procedure and were excluded from this study. Patients undergoing hairline advancement with scalp expansion or concomitant browplasty were also excluded. The 29 patients were chosen on the basis of availability of the preoperative and 1-month postoperative digital photographs.
All patients included in the study had standardized digital photographs taken by the physicians to ensure that the Frankfort horizontal plane was respected. The photographs were archived into Mirror Suite software (Canfield Imaging Systems, Fairfield, New Jersey) and analyzed using United Imaging software (United Imaging Inc, Winston-Salem, North Carolina). To obtain objective values on hairline position, we evaluated anterior-posterior and left and right three-quarter photographs. Measurements were taken in an absolute vertical orientation, and the numbers were generated from the right lateral canthus, right medial canthus, left medial canthus, and left lateral canthus to the anterior hairline. Given that all photographs were taken with the patient in repose, respecting the Frankfort plane, we believed that these positions would be the most static and give us a value that could be used to evaluate the anterior hairline position preoperatively and postoperatively. Facial height was also measured per patient from the an anterior-posterior photograph. This was defined as the point from the menton to the anterior hairline in the midline in an absolute vertical orientation. Numbers were generated from photographs, and then data were recorded into a spreadsheet (Microsoft Excel software; Microsoft Corp, Redmond, Washington). We obtained mean values per patient and then used a 2-tailed, paired t test to evaluate preoperative and postoperative averages for statistical significance in the change of hairline position as measured from the change in facial height.
Because the initial analysis did not reflect the true advancement of the hair-bearing scalp over the curvilinear skull, we performed an additional analysis. Lateral photographs taken
preoperatively and postoperatively were aligned on the Mirror Suite software. The analysis was performed using the layout board feature to align the glabella, pupils, subnasale, and stomion to ensure appropriate magnification. After printing the images, we used a flexible tape measure to determine the distance from the glabella to the trichion preoperatively and postoperatively and expressed the result as a percentage change.
PREOPERATIVE EVALUATION
Preoperative evaluation for hair direction, frontotemporal points and recessions, and adequate scalp laxity was crucial in selecting suitable candidates and counseling them. Tight scalps could have only limited lowering without scalp (tissue) expansion. To determine adequate scalp flexibility during the preoperative consultation, a point is chosen below the hairline and pushed as a high as possible (Figure 1). This point of the fingertip is set to 0 at the hairline. The fingertip is then pushed as far downward as possible and a measurement is taken. For example, 2 cm (average scalp laxity) of excursion typically allows for 2 cm of hairline advancement.
Patients with a cowlick are told that the scar at the edge of posterior growing hair will likely require hair transplants with fine follicular unit grafts for optimal results. The same is true for those wanting filling of deep temporal recessions or forward advancement of the acutely downward-growing temporal hairs. The risks and potential complications of the procedure are discussed with the patients, including telogen effluvium, visible or widened scar, bleeding, infection, the need for further scar camouflage through hair grafting or scar revision, and potential visibility of the scar with future hair loss. All patients are told to expect 6 to 12 months of diminished sensation of the frontal scalp.
First, an irregularly irregular trichophytic incision is marked in the anterior hairline for the eventual trichophytic incision. We have found it is helpful at the time of drawing the initial incision to draw parallel markings at 5-mm intervals down the forehead. Laterally, the marking fades posteriorly as the temporal recessions are approached bilaterally. Within the temporal hair, the marking extends backward and then downward for about 2 cm. We try not to mark an incision that transects the posterior branch of the superficial temporal artery. Within the temporal hair, the incision is made parallel to the hairs.
OPERATIVE TECHNIQUE
After oral premedication, the patient is taken to the operating room and given intravenous sedation, followed by local anesthetic nerve blocks and tumescence injection. This trichophytic incision is made within the fine hairs of the anterior hairline.3,7,8 This is not a pretrichial incision, as the beveling is critical and is made at about 90 ° to the exiting hairs. This allows hair growth through the scar and ensures future camouflage (Figure 2 and Figure 3). The beveling is only through the initial 2 to 3 hairs behind the point where there is a transition from fine lanugo-type hair to the thicker and denser frontal hair follicular units. The incision is carried down through the galea transecting the supraorbital and supratrochlear nerve branches and vessels. With tumescence, there is minimal bleeding. Extensive undermining in the subgaleal plane to the nuchal ridge is performed. This is a bloodless plane and is developed quickly. Galeotomies can be performed if needed for greater advancement. 9 These should be created with a depth controlled No. 15 blade. As a general rule, each galeotomy will add 1 to 2 mm of advancement. Often, several parallel galeotomies may be needed. 4 The depth of the galeotomies should be only to the point where some fat is seen. This is the point where maximum advancement will be obtained from each galeotomy but where the blood supply to the flap, which is just superficial, will not be compromised. Anteriorly, the forehead skin is undermined in the same subgaleal plane, 1 to 2 cm past the marked desired hairline. A complete forehead flap is developed only if a concomitant brow-lift is to be performed. If this is the case, then upward advancement of the forehead flap can be performed in the standard fashion for a brow-lift and fixed to the skull at the desired level.
The scalp flap is then advanced, and the amount of overlap is determined with the D’Assumpc ¸aËœo clamp or a similar flapmarking device. Once it is determined how much the scalp can be advanced, an incision is made along one of the premarked lines. This incision is made with a matching bevel to the original trichophytic incision. Non-hair-bearing forehead skin, including the galea/frontalis, is then excised. Two paramedian fixation devices (Endotine; Coapt, Palo Alto, California) are placed in the skull at about 2 to 3 cm above the new hairline; however, if a single Endotine is used, an exact sagittal location is avoided. The devices are placed in a reverse direction to their usual placement with brow-lifting, and two 5-prong retractors are used to provide tissue creep for several minutes before engaging the scalp flap onto the devices. The wound is then closed in layers using 4-0 and 2-0 polydioxanone sutures to reapproximate the galea and to avoid placing tension on the skin closure. Meticulous attention is paid to the skin closure, often using magnification to ensure proper overlap of the beveled forehead skin over the denuded hair follicles from the trichophytic incision.
RESULTS
Twenty-nine women who sought treatment for a high forehead were included in the study. Their ages ranged from 21 to 65 years, with an average age of 28 years. The women displayed a range of ethnic backgrounds, including 20 who were white (69%), 6 Asian (21%), 2 African American (7%), and 1 Hispanic (3%). Two patients had a history of endoscopic brow-lift with posterior displacement of their hairline, leading to their interest in advancing the hairline. Patients were followed up from 1 month to 8 years.
COMMENT
Much attention on rejuvenation of the upper third of the face has focused on the position of the brows and the dynamic rhytids. As a result, the position of the anterior hairline is often overlooked or ignored. Despite this, women with high hairlines will seek treatment because their large forehead makes them look more masculine and older than their years, and they lack facial harmony because of their unbalanced vertical thirds.4 This hairline advancement procedure is an effective and safe technique to correct the high female hairline in these patients.
We were able to measure an average of 1.3 cm of hairline lowering using this computer study in patients with average scalp laxity based on anterior views. This number does not reflect the amount of true advancement because it does not take the forehead curvature into account. As a result, we analyzed the profile view, and a greater degree of hairline lowering was realized (14.6% vs 23%). A percentage change of 23% or 2.1 cm is closer to the average advancement that is typically achieved at the time of surgery (range, 1.4-3.0 cm). The procedure was associated with no serious long-term complications, and all of the patients were extremely satisfied with the final cosmetic outcome and scar, even as far as 10 years postoperatively. All patients had hypoesthesia of the frontal scalp for 6 to 12 months after surgery.
Because this technique relies on an incision at the anterior hairline, it is critical to distinguish between a trichophytic and a pretrichial incision. 10 The terms are confusing and often mistakenly used interchangeably. 11 The trichophytic incision, first described by Mayer and Fleming, 7,8 is made within the fine hairs of the anterior hairline and is made perpendicular to the anterior growing hair. 12 The beveling is critical (Figure 2). The hair shaft will be cut just beneath the surface of the epidermis, and the hair bulbs will be left intact and untraumatized. Over time, as hairs begin to grow through the scar and as the hairs grow longer, future coverage and camouflage of the scar result. 1,2,4,5 If the incision is beveled too steeply, then too many hairs are transected and there is a higher chance of hairs getting trapped under the skin, leading to more cyst development postoperatively. The bevel within the temporal hair changes to parallel the hair follicles. This change prevents injury to the hair follicles and gently curves inferiorly at its distal end to lessen standing cone deformities. 5,10 Cowlick formation may make the trichophytic incision less effective on the areas where hair growth is directed posteriorly or laterally. The hairline does not start abruptly, so the incision starts just anterior to the point where there is a consistent density of follicular units. 4,5We enhance the invisibility of this incision by making it in an irregularly irregular nonrepeating pattern. The unpredictable undulations within the hairline further blend it and disguise it from the discerning eye, and the incision becomes virtually invisible1,4,5,7 (Figure 3). Exaggerated zigzag incisions should be avoided. The scar, which could become a criticism or a limitation of this procedure, becomes minimized.
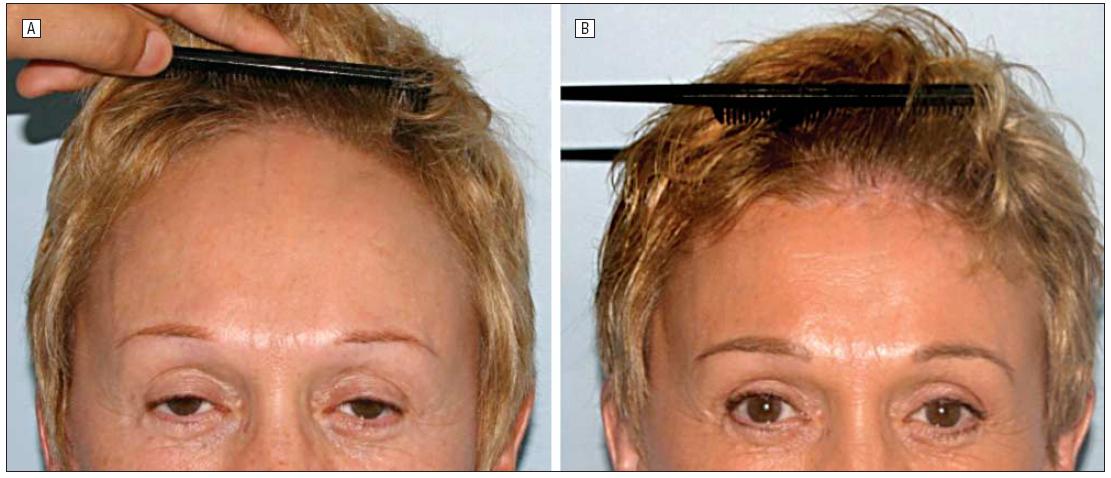
Figure 4. Preoperative photograph (A) and postoperative photograph taken 3 years after the hairline-lowering procedure (B) in a study patient.
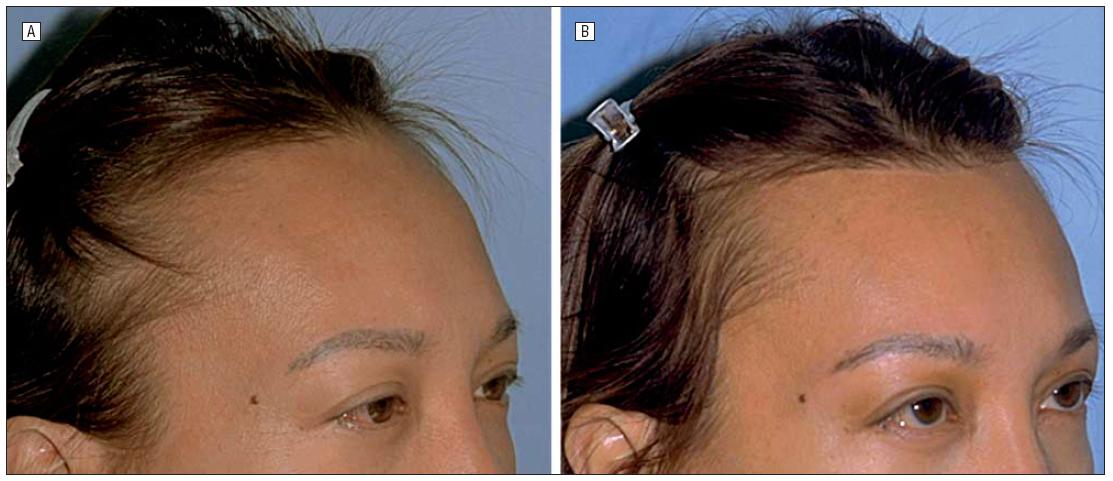
Figure 5. Preoperative photograph (A) and postoperative photograph taken 2 years after the hairline-lowering procedure (B) in a study patient.
In contrast, a pretrichial incision is made parallel to the growth of the hair3 (Figure 2). Hair shafts are not cut and hair length is undisturbed. Although this incision may be used at the hairline or within the hairs of the scalp, this incision often becomes more easily identified over time because it is seen as a linear scar with hair behind it. The pretrichial scar is often made more visible because of exposure to the sun8 (Figure 8). When used at the anterior hairline, a pretrichial incision would require bangs for coverage. Because the goal of the procedure in patients with high hairlines is to enhance the hair styling options so that bangs are not always required, this would be less than ideal. A properly executed irregular trichophytic incision can help achieve this goal.
The pretemporal incision as performed by Guyuron and Rowe,9 with a trichophytic hairline incision, preserves more of the superficial temporal blood supply to the flap and advances the temporal hairline but has its aesthetic consequences.11 Therefore, we turn our incision within the temporal hair and perform follicular unit hair transplants to the temples or temporal recessions when indicated. We thus advocate hair grafting to advance the acutely downward and posteriorly growing temporal hair for maximum cosmesis. This article studied patients with adequate scalp laxity for a single-stage procedure. However, if there is limited scalp mobility or if more than 3 cm of advancement is needed, the procedure is then staged and a subgaleal tissue expander is used. A round, 14- to 15-cm balloon expander, commonly used for breast reconstruction, is placed during the first stage. 13 Typically, an incision is made in front of the existing hairline, and a subgaleal pocket is developed toward the crown. The pocket should be sufficiently large to accommodate the expander and allow for some movement while the expander repositions itself during the initial injections. Galeotomies can be made to allow for more rapid expansion.12 The injection port is placed in the temporal area so that it can be easily found during the weekly injections. The incision is then closed in 2 layers. Approximately 100 mL is injected into the expander at the end of the case. This allows the expander to unroll any curled edges that occurred during placement and allows for palpation and localization of the expander.
Figure 6. Preoperative photograph (A) and postoperative photograph taken 4 years after the hairline-lowering procedure (B) in a study patient.
Figure 7. Preoperative photograph (A) and postoperative photograph taken 21â„2 years after a hairline-lowering procedure with a brow-lift (B).
Ptotic brows could also be easily managed at the same time as the hairline advancement14 (Figure 7). The approach is similar to that of standard open brow-lifting techniques. 15 On the other hand, 2 patients who had undergone previous endoscopic brow-lifting with resulting elevation of their hairlines were also excellent candidates for this procedure. Despite their brows being in a good position, they did not like the change in their hairlines, and their enlarged foreheads became an issue that required attention (Figure 4).
Other surgical options exist for patients with high hairlines. Hair transplantation using a follicular unit grafting technique is an effective treatment that has a low incidence of complications and is considered the gold standard for hair work. However, this technique is labor intensive, is time consuming, and can be expensive, especiallybecause these patients would require multiple sessions to achieve the significant hairline lowering required with adequate density. In addition, female patients will have to wait 2 to 4 years to see the full results of the transplantation. We believe that, when it is an option, the described hairline-lowering/scalpadvancement procedure has substantial advantages over transplantation. However, follicular unit grafting can be used as a complement to this procedure for further scar camouflage.
In conclusion, we describe herein a technique that has been used by the senior author (S.S.K.) effectively to treat female patients with a high hairline. The technique produces outstanding results rapidly, is readily acceptable to patients, and has few significant complications. We believe the hairline advancement technique is a valuable tool to add to the armamentarium of the facial plastic surgeon. We attempted to perform a scientific statistical study of a clinical technique that gave us data that we hope have added to information on this relatively rare but gratifying procedure for the patient and the surgeon.
Accepted for Publication: August 28, 2008.
Correspondence: Sheldon S. Kabaker, MD, Aesthetic Facial Plastic Surgery Medical Clinic, 3324 Webster St, Oakland, CA 94609 (Hairflapmd@aol.com or Kevinende@comcast.net).
Author Contributions: Study concept and design: Ramirez, Ende, and Kabaker. Acquisition of data: Ramirez, Ende, and Kabaker. Analysis and interpretation of data: Ramirez, Ende, and Kabaker. Drafting of the manuscript: Ramirez, Ende, and Kabaker. Critical revision of the manuscript for important intellectual content: Ramirez, Ende, and Kabaker. Statistical analysis: Ramirez, Ende, and Kabaker. Administrative, technical, and material support: Ramirez, Ende, and Kabaker. Study supervision: Kabaker.
Financial Disclosure: None reported.
Previous Presentation: This Facial Plastic Surgery Fellowship paper was presented at the American Academy of Facial Plastic Surgery Fall Meeting; September 25, 2005; Oakland, California.
REFERENCES
Sheldon S. Kabaker, M.D.
—
Bill Seemiller
Associate Publisher/Editor
Technorati Tags: hairline lowering, high forehead, Dr. Shelly Kabaker, high foreheads, female hairline, high forehead, high foreheads, hair density, high hairline, high hairlines, large foreheads, scalp laxity, hairline-lowering procedure, hair loss, brow-lifts, alopecia, hairline advancement, scalp expansion, follicular unit grafts, telogen effluvium, hair grafting, scar revision, future hair loss, trichophytic, hair growth, effluvium, shock hair loss, Hair transplantation, follicular unit grafting
I'm at thirty-one year old man with a Norwood 6 level of hair loss. I…
I'm a 31 year old male I have been losing hair for the past six…
I'm concerned that i'm going bald. My dad is 54 years old, and still has…
I'm a 30-year old male with a Norwood 4 hair loss pattern. I have been…
I'm twenty years old and already have aggressive hair loss. I'm imbetween a Norwood 5…
I'm interested in getting a hair transplant later this year, but I am a very…
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
View Comments
Im looking for some body to push up my narrow and small forehead. since im a man i think that i need a broder and higher forehead because it makes the men face more attractive. can you please ask the doctor if its possible to push up the forehead hairline and make the head look with a broder and higher forehead
Do you know of any surgeons in North Carolina or South Carolina that perform this procedure?
Zara,
Unfortunately, I'm not aware of any physicians in the Philippines performing this procedure. However, we do recommend a number of excellent hair transplant surgeons in the surrounding areas. To see a list of physicians we recommend, click here. To see our demanding standards for recommendation, click here.
Note that many hair loss patients travel great distances to have the very best doctors provide them with world renowned results.
Good luck!
David
Hi, I'm Zara. Is there any trusted doctors who does the same procedure here in the Philippines?
Cecilia,
I'm not aware of any clinics performing the female hairline lowering procedure in Brazil. However, I suggest contacting recommended hair transplant surgeon Dr. Arthur Tykocinski in São Paulo.
If his clinic does not perform this procedure, they may be able to refer you to one that does.
Good luck!
David
Hi,
i´m from brazil and would like to know if you can recomend some professional that could do this surgery here, and about how much will it cost.. just to get an ideia of values.
thanks!
alisha,
I'm not aware of anyone in India performing forehead reduction surgery. However, you may have success in contacting one or both of the hair transplant surgeons we recommend in India. They may perform the procedure and, if they don't, they may be able to recommend a clinic that does.
Dr. Pathuri Madhu
Dr. Radha Palakurthi
Good luck!
David
Good luck!
David
I hv a big forehead .. its smaller on both the sides.. But bigger in between.. N also my skin is too sensitive..m lukin forward to this surgery bt very much scared abt the side effects.. I liv in delhi.. Can ne body recommend me any doctor here only and also the cost? Plz help
Please can someone tell me if they have succesfully had hairline lowering procedure done in the Uk.....?
Ann,
You could definitely contact Dr. Kabaker and see what type of arrangements he can make for international patients. Please see his recommendation profile for his contact information: http://www.hairtransplantnetwork.com/Consult-a-Physician/doctors.asp?DrID=138#page=page-1.
Additionally, if you're interested in seeking the advice of hair restoration physicians in Europe, please see our European recommended hair transplant surgeons: http://www.hairtransplantnetwork.com/Consult-a-Physician/hair-loss-doctors-europe.asp
Good luck!
Blake (Future_HT_Doc)
Editorial Assistant