Overview of the 2014 ISHRS Meeting
FUE-related presentations included: a discussion of FUE-based Body Hair Transplantation (BHT) from Coalition hair transplant surgeon Dr. Robert True and recommended hair restoration physician Dr. Sanusi Umar; an overview of “treading the FUE path” – or FUE pearls and pitfalls – by recommended physician Dr. Tejinder Bhatti; a presentation on beard hair FUE (a specific type of Body Hair Transplantation) again by Dr. True; a discussion regarding the role of the dull punch in Follicular Unit Extraction given by FUE pioneer and recommended physician Dr. James Harris; a presentation on the challenges of performing FUE in African American patients by Dr. Umar; a discussion about selecting the “right” FUE tool and avoiding graft transection by Coalition physician Dr. Jean Devroye; and an exciting course on the use of manual FUE extraction tools taught by Dr. Jose Lorenzo.
Other interesting presentations included: a talk on designing patient hairlines – featuring Coalition physician Dr. Damkerng Pathomvanich discussing Asian hairline design and Coalition physician Dr. Ron Shapiro discussing Caucasian hairline design; an overview of the most effective graft storage solutions available for hair transplant surgery – featuring a presentation advocating for the use of Hypothermasol by Coalition surgeon Dr. Jerry Cooley and a presentation discussing Plasmalyte from Coalition physician Dr. Timothy Carman; a presentation examining the role of hyaluronidase for taking larger strips with less scarring in FUSS procedures by Dr. True; a presentation on the use of platelet rich plasma (PRP) in hair transplant surgery; and an update on “future” hair loss treatments.
Background on the ISHRS
At the meeting, Coalition member Dr. Sharon Keene replaced Dr. Vincenzo Gambino as the acting President of the ISHRS for the coming year. Congratulations to Dr. Keene for receiving this honor.
Physician Recognition and Awards
Congratulations to the following award recipients:
Recommended hair transplant surgeon Dr. James Harris was awarded the Golden Follicle Award for his role in developing innovative hair restoration techniques and furthering the advancement of hair restoration.
Dr. Ken Washenik won the coveted Platinum Follicle Award for his outstanding achievements in basic science and clinically-related research in hair pathophysiology and anatomy.
Congratulations as well to Dr. Russell G. Knudsen for winning the coveted Manfred Lucas Award for his many contributions to the advancement of physician and staff education.
This year, the Distinguished Assistant Award went to Lauren “Laurie” Gorham, RN of Dorchester, Massachusetts. Laurie Gorham works for Bosley.
Presentations of Interest to Hair Loss Sufferers
Below are the highlights of exciting presentations from our recommended and Coalition physicians – and other hair loss experts – at the 2014 ISHRS conference:
Hairline Design: the Right Hairline for the Right Patient
According to Dr. Pathomvanich, Asians possess unique skull shapes with less forehead projection and different facial features. This requires a “flatter” more “U-shaped” hairline design. Many hair restoration physicians don’t realize this, and drawing a traditional Caucasian hairline on an Asian patient often results in poor facial framing.
Graft Storage Mediums: Best Way to Store Grafts During Hair Transplant Surgery?
Role of Body Hair Transplants (BHT) in Modern Hair Restoration Surgery?
Recommended physician Dr. Sanusi Umar – a body hair transplant pioneer – agrees, and frequently tries to improve the use of body hair transplants in new and innovative ways. One of his new discovers involves a novel approach to eyelash restoration: using leg hair follicular unit grafts for eyelash transplant surgery. Dr. Umar noted that the naturally short and curled leg hair follicles mimic eyelash hair, and concluded that leg hair follicles could be useful in eyelash transplantation.
He tested his theory by comparing two patients: one who underwent eyelash transplantation with scalp follicles and another who underwent surgery with leg hair follicles. After 3 months, both patients had a yield of 80-85%. The scalp follicle patient required eyelash trimming every 2 weeks and used mascara and curlers to shape the lashes. The leg hair patient, on the other hand, required no trimming and noted effective shape and curl in the transplanted lashes without the use of mascara and curling tools. Dr. Umar believes eyelash transplantation with leg hair follicles may represent a new use of body hair transplants.
To review the results of this case, please see the following: FUE Eyelash Transplant with Leg Hair.
Role of the Dull Punch in FUE
Hyaluronidase in Follicular Unit Strip Surgery (FUSS): a Safe Way to Take Large Strips with Less Scarring?
After being introduced to the technique by Dr. Cooley, Dr. Robert True began using hyaluronidase in his practice. Dr. True routinely began injecting the donor regions of patients with hyaluronidase before strip extraction. He used this technique in three specific patient populations: individuals seeking the largest strip harvest possible; patients with a previous donor scar; and patients with inelastic scalps. Dr. True has injected over 150 patients with hyaluronidase before strip extraction. After reviewing the results, Dr. True observed the following: hyaluronidase typically increased strip harvest by 20-50%; despite increased strip widths, the resulting donor scars were typically 1mm (+/-) wide; and while less than 5% of patients noted increased temporary shedding in the donor region, no long-term complications were revealed. From this, Dr. True concluded that using hyaluronidase in strip procedures is an effective way of increasing strip width and maximizing harvest without creating wider donor scars.
Future Hair Loss Treatments: Is Bimatoprost (Latisse) the Next Treatment for Androgenic Alopecia (AGA)?
Treading the FUE Path: Pearls and Pitfalls: Dr. Tejinder Bhatti
Introduction
Those who have followed the development and evolution of hair transplantation tools and techniques over the past few years know that follicular unit extraction (FUE) is becoming increasingly popular among hair loss sufferers seeking surgical hair restoration. This is due, in part, to the fact that FUE is less invasive than follicular unit strip surgery (FUSS) and the lack of a linear strip scar offers the potential to wear a close cropped haircut. However, the real catalyst for this recent explosion of interest in the procedure may be that FUE practitioners have worked diligently to increase the efficacy of the procedure. Today’s FUE sessions can exceed 2,000 grafts in a single day when appropriate for the patient, with a high rate of success; a feat unheard of only a few short years ago.
Substantiating Data:
This presentation is the result of my 3 year experience of 1518 cases of FUE since September, 2010 when we at the clinic made the complete transition from follicular unit strip surgery (FUSS) to FUE after realizing the safety, effectiveness and patient friendliness of the technique. We use blunt Harris punches which may vary in diameter from 0.65-0.85mm in diameter. Only mechanical (motorized) extraction is done using the Safe Scribe system of Dr. James Harris. The peer certified rate of extraction varies from 1200 to 2000 per hour (average 1400). As we have trained over 220 doctors from India and abroad in FUE technique, our technique stands peer reviewed and so do the facts we reveal.
Discussion:
Bad results or disasters ensue after a hair transplant due to one or more of the following reasons:
These 3 cases were done in 2011 using FUE technique with large diameter punches of size 2 mm resulting in a classic doll’s head look, pitting of grafts, low density and an overall unaesthetic look.
Visible scars with sequestration cyst formation. Scars due to use of 2 mm punches, which are very much in use today, under the garb of FUE. Cysts form due to improper inspection for buried grafts at the end of the harvesting.
Large punch size resulting in prominent scarring in the donor area.
Malpractice – “100 free grafts Trial”- This patient is a victim of an aggressive “promotional offer”. The grafts have been placed in such a strategic position that the patient has
The posterior hairline has been deliberately formed in a straight line to make it look artificial so he returns for the next procedure sooner than 6 months.
Conclusion:
If you believe that FUE is the oldest surgical hair restoration procedure, we have come full circle. Gone is the era that associated punch grafting with bad pluggy, doll-head results. Today’s FUE is a refined procedure that utilizes miniscule punches which range in size from 0.65- 0.85 mm to provide an undetectable, natural result with high density without leaving a visible linear scar. As a prominent FUE learning center in Asia, Dr. Bhatti in India realized and projected 3 years ago the force of FUE, its wide acceptance being minimally invasive in nature, and the value it brings to the field of surgical hair restoration. Having trained over 190 doctors in the past 3 years alone, he never came across a doctor who would have liked to learn strip as well after seeing the potential of the procedure to harvest a large number of grafts in a single session. The decline of strip is mostly related to the linear scar which gets broader and therefore more visible after each repeat session. No amount of trichophytic closure or w-plasty can make it invisible when sporting no.1 or 2 size hair. It was a conscious decision to switch over to FUE keeping in mind the increasing demand of the procedure in India amongst a population which is wary of surgical techniques for cosmesis. However, Dr. Bhatti continues to offer the strip method to patients with-
It has been Dr. Bhatti’s experience that even this miniscule subset of patients would rather have grafts harvested from their beard, chest, etc. rather than live with a visible linear scar all their lives.
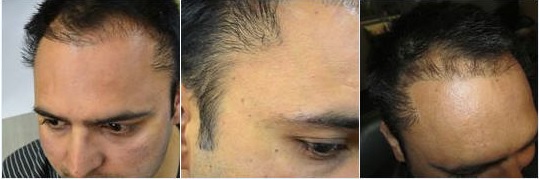
FUE in African American Hair: Dr. Sanusi Umar
Normally, with a great deal of difficulty, conventional FUE punches would be successful in 10-30% of patients with afro-textured hair. Dr. Umar has worked for over 6 years developing a device and method that can successfully tackle even the kinkiest hair and he succeeded with this tool,which also has a version for patients with straight hair and loose wavy hair as well.
Patients Presented
Case 1: A patient who had recorded over 60% transection with all conventional methods of FUE including several test procedures at Dr. Umar’s clinic. He was seen by another physician in Beverly Hills who presented as having FUE success in this demographic. Unfortunately, his yield was very poor and now had significant FUE scarring in the head donor area that increased the difficulty level of any future FUE procedure. The new tool and method presented at the 2014 meeting in Kuala Lumpur was highly successful with a transection rate of less than 10%.
Case 2: FUE test using Dr. Umar’s existing rotary punches showed transection rates of over 50%. The new tool and method performed with a transection rate of less than 5%
Conclusion
Unfortunately, the details presented at this year’s ISHRS meeting are currently classified pending publication of the work in a scientific peer-reviewed-journal. There are also proprietary matters as well as data collection expected to be completed before January 2015. These tools should be made available at the next ISHRS meeting in Chicago to interested FUE practitioners. Dr Umar has already proposed (to the next meeting chair) a live workshop to teach methods of use to attendees at the 2015 meeting.
ARTAS: Robotic Recipient Site Creation: Dr. Robert Bernstein
Introduction
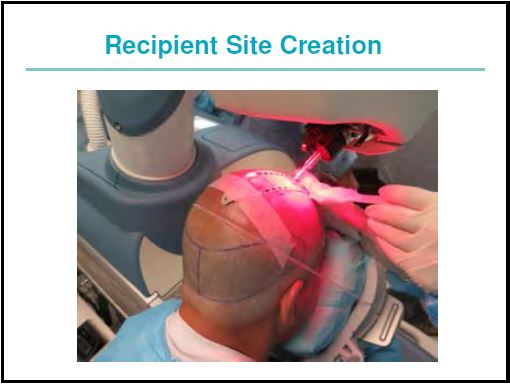
The first robot to assist in follicular unit transplant procedures was released in the fall of 2011. The initial application was the in-vivo separation of follicular units from the surrounding scalp tissue. With new hardware and software capabilities, the robot can now create recipient sites. Preliminary observation suggests that it can perform this function with greater precision and consistency than can generally be accomplished manually.
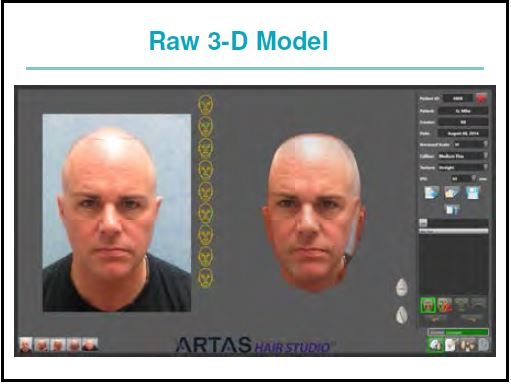
Method
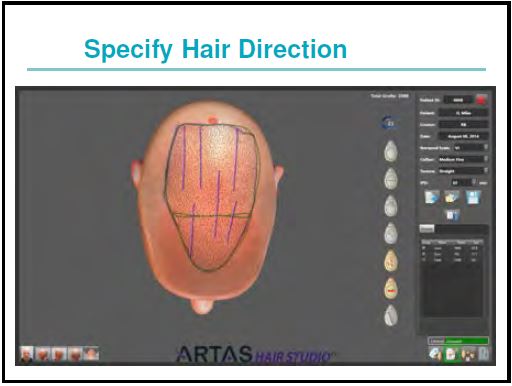
For robotic recipient site creation, the doctor first draws a hairline and other markings directly onto the patient’s scalp to delineate the area to be transplanted. Next, multiple photographs are taken of the patient and software converts the images and markings into a 3-D model of the patient.
The physician then specifies the angle of hair elevation and direction, average density, total number of the recipient site incisions and recipient site depth. The robotic device uses image-guided technology to avoid hairs of a specific diameter. In this way, the new distribution of sites can be made to complement the distribution of existing terminal hairs (or the hair from prior hair transplant procedures), while at the same time ignoring hair that is miniaturized or vellus.
The imaging software for site creation can be used as an integrated system for both designing the restoration at the consult and guiding the surgery. It also can be used independently as a consulting tool, or in the OR guiding the creation of recipient sites.
Conclusion
In performing recipient site creation, the robot automates another part of the hair transplant process that can be prone to human variability and error. The new technology also gives the physician a tool at the time of the consult to show what the hair restoration procedure can do and to better align the patient’s expectations with anticipated results.
Low Level Laser Therapy (LLLT): How Does it Work? What is the Difference Between the Different Devices?
Dr. Keene has found that beaming laser or any other light on to hair seems unlikely to get to scalp. Only very thin hairs will allow the light to penetrate if the scalp is exposed properly. If light is not perpendicular to the scalp or not touching the scalp, it is likely not to work well or at all. This means that laser hoods and overhead devices cannot make the same claims that devices such as the HairMax LaserComb that touch the scalp do. Also, there are fundamental flaws in recent LLLT studies. Their hair counting methods appeared to be inaccurate so results are not reliable (except the laser comb–but results were modest and no one knows if they are sustainable).
Meeting Conclusion
The fields of medical and surgical hair restoration continue to develop and improve thanks to the efforts of skilled and experienced hair restoration physicians like those recommended on The Hair Transplant Network.
We would like to extend our thanks to those physicians who attended this year’s ISHRS meeting in San Francisco and contributed to the writing of this presentation.
Technorati Tags: 2014 ISHRS Meeting, International Society of Hair Restoration Surgery, ISHRS, hair loss, hair restoration, Follicular Unit Extraction, FUE, future hair loss treatments, Follicular Unit Strip Surgery, FUSS, hair transplant, Asian hairline design, Caucasian hairline design, graft storage solutions, hair transplant surgery, platelet rich plasma, PRP, Dr. Damkerng Pathomvanich, Dr. Ron Shapiro, Dr. Timothy Carman, Plasmalyte A, Dr. Jerry Cooley, Hypothermasol, graft storage, Body Hair Transplants, BHT, hair restoration surgery, body hair transplant, eyelash restoration, eyelash transplant, Dr. James Harris, SAFE FUE, Hyaluronidase, HRH, bimatoprost, Latisse, PGD2, androgenic alopecia, hair transplantation, Dr. Tejinder Bhatti, Dr. Sanusi Umar, Dr. Robert Bernstein, Low-level laser treatment, hair growth, hair loss treatments, Dr. Sharon Keene, HairMax LaserComb
I'm at thirty-one year old man with a Norwood 6 level of hair loss. I…
I'm a 31 year old male I have been losing hair for the past six…
I'm concerned that i'm going bald. My dad is 54 years old, and still has…
I'm a 30-year old male with a Norwood 4 hair loss pattern. I have been…
I'm twenty years old and already have aggressive hair loss. I'm imbetween a Norwood 5…
I'm interested in getting a hair transplant later this year, but I am a very…
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}