Managing Crown Hair Loss through Hair Transplant Surgery
This insightful article was written by hair loss physician Dr. Jean Devroye, who is a member of the Coalition of Independent Hair Restoration Physicians.
 Synopsis
Synopsis
Hair transplantation at the level of the vertex is not an easy to manage technique. This article, after having revised the notions of anatomy, describes the strategic stakes which are necessary to face. It also gives numerous details on the technique to implement in order to obtain the most natural result possible and which also gives the best possible apparent density.
Introduction
The vertex is a complex zone. The hairs are arranged in a radial way. It is of course subject to more or less complete baldness. The progression of this is mostly eccentric, starting from the center and evolving more or less quickly towards the periphery.
It is no easy task to treat the vertex for several reasons that will be developed hereunder.
We are often in an uncertain situation, facing a progression the outcome of which we do not know and the hair loss is often widespread. The thinning often includes the frontal zone, the midscalp and the vertex. It is essential to take into account the Donor-Recipient Area Ratio. Unfortunately this ratio is transformational. It’s never easy to choose the best strategy knowing the vertex is a secondary zone by comparison with the anterior and median zones.
I shall describe exclusively the vertex alopecia in males. Indeed, it is exceptional to treat vertex balding in women. In fact, women almost never have enough graft reserve to treat the vertex.
Anatomic Description of Vertex: (fig 1)

Fig 1 Vertex transition point
The vertex means literally “the highest point”. It is a round or oval zone, surrounded at the back and on the sides by the borders of the permanent zone. It is defined as the most posterior part of the area concerned by male pattern baldness. Its limits are the midscalp on the front and the parietal and occipital fringe on the back and on the sides. Hair is arranged there in a whorl or swirl, starting from one or two centers. (1)
In order to define the limit between the midscalp on the front and the vertex on the back, we use an anatomic mark named the vertex transition point. The vertex transition point is the point where the horizontal part of the skull starts sloping downward to become oblique and then vertical towards the back. From this point, we draw a concave curved line downward which joins the side limits. It is not always easy to locate this point because the surface of the skull is often round without any real point of visible transition. Unger (2) writes : « Also, in most men with Type IV and Type V MPB, the anterior outline of the vertex area usually naturally ends at the posterior border of the “mid-parietal bridge,” or the remnant thereof. In the majority of men with vertex Type III as well as Types IV and V MPB, this designated “vertex” area occupies the classic“tonsure” position, thus straddling both the horizontal and vertical planes of the scalp. In balding men with the more severe Norwood Types VI and VII patterns, the vertex has a large, circular (or somewhat oval) shape that rather than straddling both the horizontal and vertical planes, occupies essentially only the vertical plane. This is because its posterior border extends further inferiorly than in Types IV and V, and, therefore, the anterior border of its anterior mirror image is farther posterior than in Types IV and V MPB.”
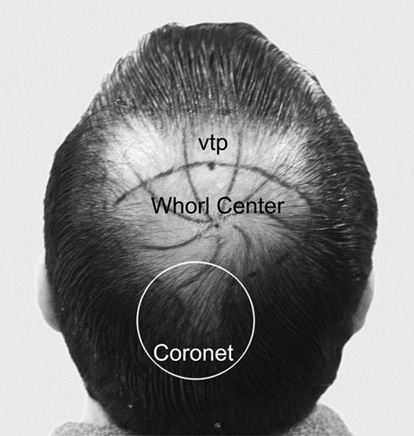
Fig 2 Vertex transition point, Whorl center and coronet
Pay attention that the transition point does not correspond to the center of the whorl. It is situated some centimeters above. It will be necessary to be precise when we talk about the treatment of the “vertex” or “crown”. Indeed, a transplant of the posterior part of the scalp, centered on the whorl, often includes not only the vertex, strictly speaking, but also the posterior part of the midscalp.
The posterior and side edges of the vertex, that are the parietal and occipital fringe, do not correspond to anatomically precise entities because they are at the transitional limit between the thinning zone and the hair bearing area. These borders are a very important area because they are moving.
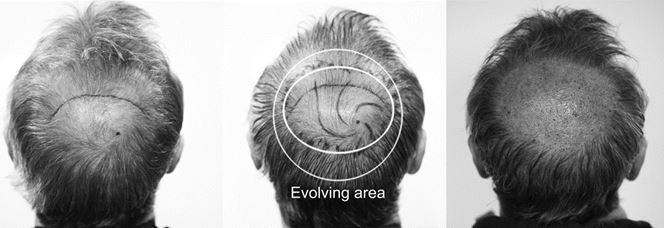
Fig 3 Limit of the balding area with dry and wet hair
It is extremely useful to try to foresee as precisely as possible the future peripheral limit of the balding of the vertex. Indeed, the current surface to be transplanted or the potentially bald one is often very large. When the baldness is advanced, we can determine rather sharply, the place where the hairs of the donor zone give way to largely miniaturized hair. When the balding is incomplete, it is often easier to determine this limit in a macroscopic manner by wetting hair and by using a good light to visualize the skin through the hair. This region is often named “the evolving area”. (fig 3)
There are some anatomical variations, in particular the existence of two swirl centers. There is often a small area of loss in the low part of the occipital fringe, inferior to the larger “crown” pattern, which James Arnold named the coronet (3) (fig.2)
It is important to take the coronet into account. Indeed, it encroaches and thus reduces the “safe” donor zone.
The exit angle of the hair compared with the skin is variable too, high in the center of the swirl, it becomes lower to the periphery.
How does the vertex baldness evolve?
Vertex balding is a part of general baldness. Most of the time, it appears later than the balding of the anterior and midscalp zones.
According to the age of the patient, hair loss on the vertex is more or less important. It is effective in stages III vertex, IV, V VI and VII of the Norwood scale.
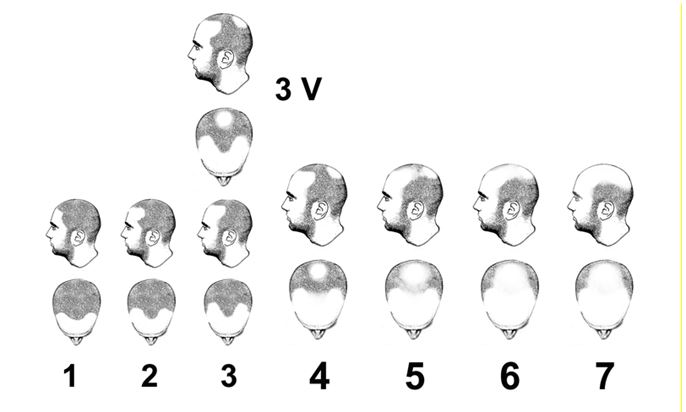
Fig 4 Norwood classification
According to the Norwood study (4):
- Between 18 and 29 years old, only 6% of Male Pattern Baldness is related to the vertex.
- Between 30 and 39 years old, 21%
- Between 40 and 49 years old, 30 %
- Between 50 and 59 years old, 37 %
- Between 60 and 69 years old, 53%
- Between 70 and 79 years old, 50 %.
The study of Unger shows a prevalence from 65 to 73 % above 60 years old. (5)
It sometimes happens that the patient loses his hair essentially at the level of the vertex.
The hair loss of the vertex begins mostly from the center to propagate towards the periphery. It evolves in the form of a circle or an oval which grows gradually towards the outside. The surface of a circle evolves exponentially with the increase of its diameter. It is the reason why it is necessary to be very cautious when we judge unfinished hair loss. The surface of an emptied vertex of 5cm in diameter is going to quadruple when it grows to a diameter of 10 cm.
Clinical Examination
It is thus very important to observe exactly the situation of the vertex before any decision-making. The use of the cross section trichometer of Dr Cohen is deeply recommended. (6) It allows quantifying quite exactly the scale of the loss. Also a fine observation of the emptied zone through quality magnifying glasses of magnification 5 or 6 is widely recommended. We shall try to define the topography of the miniaturization in these area.
We shall mostly try to highlight the thinning of the peripheral zone which frequently begins several years before definitive balding. To wet hair and to use a strong light is often an effective method. Unfortunately, before the ages from 40 to 50 years old, it is often virtually impossible to predict with an absolute certitude which will be the degree of balding reached. It is necessary to be aware of it and also to explain it to the patient so that he can approve, in full knowledge of the facts, the final therapeutic choice.
The vertex is not visible in the front view unless the patient is seated and slightly bowed forward. On the contrary, from profile and of course back view, the vertex baldness is visible.
Anamnesis
A precise interrogation concerning the family history is often very useful. It is necessary to try and find out the degree of balding of the vertex of the father and the grandparents and of the collateral family, keeping in mind that this comparison is not always reliable. We shall try to find a member of the family having had the same type of evolution in severity and in age.
Age Guidelines:

General Reflections about the Treatment
Requests for vertex treatment vary according to the age and the situation of the patient. The requests of a patient who presents a pattern affecting any other area than the vertex are variable. A well informed patient will tend to ask first for treatment of the anterior zone. However it is frequent to see patients who want the complete treatment of the anterior and posterior zones. It is less frequent to see a patient focusing his complaint on the vertex only, either because it is the mainly emptied zone, or for other reasons like the fear of a too radical change of aspect of the anterior area, or the fear of not having enough donor zone to cover the whole baldness.
The vertex is hidden from the view of the patient. It is rare that he has a perfect consciousness of the size of the thinning zone. He often imagines it smaller than it is. This is due to the fact that the vertex is posterior and vertical and that he rarely sees it entirely. The patient often imagines that some hundreds of grafts can solve his baldness. It will be necessary to spend time to explain clearly the situation to him. It is necessary to inform him about uncertainties regarding the evolution of the donor zone. He has to realize the limit which represents the donor-recipient zone ratio.
Patients are often very receptive to the explanations. During the first consultation, we shall detect unrealistic requests, the patients whose expectations will never be achievable. It is better to give up a surgery than to have an unsatisfied patient due to a bad diagnostic.
Therapeutic Options
Medications
The vertex is a zone which reacts relatively well to medications like Propecia (finasteride) and Rogaine (minoxidil). (7) (8). When the patient is young, and when it is difficult to estimate the progression of his hair loss, we shall prefer to use first a medical hair loss treatment. It will allow letting a few years pass before deciding which quantity of grafts we decide to allocate to the vertex. Certain hair restoration surgeons recommend systematically a one year treatment before envisaging the transplant of the vertex at a young man. It is however necessary to be aware that the success of a medical treatment is never definitive. It simply delays the inexorable occurrence of the final balding. For a young man, the stabilization of the loss through the medications does not give us at all the right to forget the various caution rules expressed in this chapter.
Scalp reduction
Only a few years ago, the scalp reduction was considered the ideal approach to reduce vertex baldness. It consists in removing an oval skin zone in the center of the vertex. The donor side zone is then polled and widened to cover the bald zone which was removed. Dr Frechet (10) improved the classic technique by the use of an extender. This one increases the surface of the removed skin. Since the success of follicular unit hair transplants at the end of mid-nineties, the scalp reduction gradually lost its indication and only some rare surgeons still use it. Its main defects are the rather drastic reduction of the density of the donor zone by stretching, which can mortgage the treatment of the anterior zone. On the other hand, the reduction leaves a scar which can widen by a stretch back phenomenon. Also the orientation of the displaced hair does not correspond at all to the original orientation; the swirl is replaced by a double side unsightly orientation. The patient cannot find any hairstyle enabling him to camouflage the unnatural appearance of the hair on either side growing in opposite directions. Dr Frechet (10) finalized the triple flap technique which partially corrects this defect.
Finally, it is a relatively aggressive, often painful intervention when extenders are used. These are the main reasons for which the patients are not favorable any more. The general evolution is rather the search for soft techniques, on the contrary. The recent advent of follicular unit extraction (FUE) is a good illustration of that.
Follicular Hair Transplant
Follicular unit hair transplantation with dissecting microscopes initiated by Dr. Bobby Limmer in 1987 and Rassman & Bernstein has revolutionized the practice of hair transplantation. It has now become the preferred surgical treatment. It avoids the pluggy appearance that characterized older grafts. It has the huge advantage of being able to work with two factors: the use of different follicle size and composition and a density and orientation variation of grafted hair. It gives a very natural result that fits perfectly in the existing hair.
Is It Wise to Operate? What Are Good Indicators?
Every surgeon reacts according to his experience, according to the peculiarities of his practice and according to his degree of caution. In his very interesting article The Paradox of Crown Transplantation ,(9) Dowling B Stought explains the “guidelines” dilemma in the particular case of vertex transplantation. Indeed, it is not easy to find infallible rules. There are numerous exceptions. The danger of guidelines for the treatment of the vertex is that they could then be used against the surgeon who would have made a bad strategic decision. This is why it will always be necessary to be extremely careful before deciding to practice transplantation on the vertex.
It is necessary to spend some time to explain to the patient the risks and the consequences of this first intervention. It is also necessary to prepare and to sign a precise consent form which explains clearly the uncertainties we can have as to the future hair loss of this zone.
Most of the authors are clearly reserved regarding the treatment of the vertex. They refuse to operate before the age of 35-45 years. There are however exceptions to this rule for some of them.
What are the argument in favor of surgical intervention and the rules to respect in this case?
- It is necessary to make sure that the donor is full enough to cover the crown with sufficient density. It is thus necessary to analyze four factors: the density in terms of number of hair by cm2 (hair density), the average diameter of hair, the texture of hair and finally hair color. The notion of Donor-Recipient Area Ratio is very important.
- It is often inadvisable to proceed before the age of 35 or even 40 years ( Unger) (2) or even 45 years, (Stought,Parsley) (9)
- Ideally, it is necessary to have finished the work in the anterior zones (frontal and midscalp) before deciding to treat also the vertex.
- We should not try to reach a maximal cover but rather an acceptable density to keep the donor zone for the future needs.
- The patient has to accept the risk linked to the fact that we don’t know exactly what the evolution of the ratio donor-recipient area will be.
- When we treat the frontal zone and the midscalp with desirable density, we sometimes increase the feeling of emptiness at the level of the vertex, mostly if the skin is completely bald at this level.
- The grafted zone may serve to anchor hair coming from the front and brushed to the back.
Arguments against surgical intervention.
- The vertex has very little cosmetic impact. When you look at someone, you are face to face. The aspect of anterior zones is the most important.
Bobby Limmer wrote : “The most difficult task the consulting physician faces is educating and convincing the hair loss patient that the frontal and midscalp constitutes 90 % of the value while vertex restoration produces the other 10 %.” (9) - The frontal transplants often allow obtaining enough density so that these hairs, brushed to the back, cover the vertex zone. This type of hairstyle is very natural and does not give the aspect of the artificial lock that we have when the hair is brushed from the vertex forward to cover an anterior balding area.
- When a vertex transplant has been made and as hair loss progresses, a halo of baldness could appear around the transplanted zone. If due to the lack of grafts, we are not capable of continuing to fill in the vertex, the aspect resulting from this, risks being a source of important dissatisfaction. It is made by an island of hair, lost in the middle of a completely bald area. A transplant, whatever the concerned zone, stops being natural when it is surrounded by an emptied zone. It is the biggest pitfall of the vertex transplant..
- It is often interesting to strengthen a first transplant of the anterior zone and the midscalp by a second transplant. If we start the global treatment with a transplant of the vertex, we lose this possibility of reinforcement during a second intervention.
- If the patient suffers from an already wide baldness, the treatment of the front is going to minimize his complaints concerning the vertex, all the more if he brushes his hair backwards.
- The total surface to be transplanted is often big, equal to the addition of the surfaces of the frontal zone and the midscalp combined.
- The shingling effect is less important at the level of the vertex. The shingling effect or overlapping phenomenon is very important in the frame of hair transplant.
Thanks to the covering of the hair layers one on top of the other, the “visible macroscopic density” can be sharply more favorable at the level of the frontal zone than at the level of the vertex, for the same type of work and with the same type of graft density.
The explanation is simple: given the fact that hair scatters according to a swirl, the shingling phenomenon scatters in all directions instead of concentrating in only one. This lack of overlapping is particularly important in the center of the swirl. In spite of the operating subtleties (see below), it is often useful to have a second surgery to complete the density at this level.
The Surgical Technique
The author gives here the details of his own technique. It will be illustrated in the video. There are of course other approaches that will also be mentioned.
Preparing the Recipient Area
The patient is seated, many pictures are taken. It is often very wise to make pictures from the front, with the head lowered forward. To reveal the posterior hair loss and its connection with the front, it is useful to take pictures from the back, with the head lowered to the maximum backwards.
We almost systematically shave the recipient area. We convince the patient by arguing that the shaving allows a substantial improvement of the quality of the work at all levels. Only few patients refuse. In that case, we recommend a short cutting. From time to time, we operate a vertex with long hair.
Direct lines are drawn. They follow the main trunk road according to which the existing hairs are arranged. As a general rule, there are enough young vellus hairs to guide us in the reconstruction. We shall respect the existence of the various patterns described by Ziering. It is very rare that we have to create a new vertex center. If it is the case, we shall move this vertex center away from the normal center. If the patient wishes to comb counterclockwise, it’s better to place the center moved away to the right from the center and conversely for the clockwise direction. By placing the center relatively high, rather close to the transition line, we increase the overwhelming effect on the posterior part and, therefore, the impression of density at this level is improved.
Patient Position
We have always preferred the prone position for the removal of the strip in FUT as well as for the extractions in FUE. The work is more comfortable for the surgeon (even if it is less comfortable for the patient) and it gains in quality.
Incisions:
There are two big scenarios which will be handled very differently.
Minimalist Covering
Minimal density will average between 25 and 30 or even sometimes 20 incisions per cm2.
Several circumstances can limit the number of available grafts or more exactly the transfer of available hair mass.
It can be due to the careful decision of the surgeon to dedicate only a very limited quantity of grafts to the vertex even if the reserve of hair seems sufficient at this moment. It can also be linked to a bad donor-recipient zone ratio which reduces the number of available grafts for the vertex, or to a low average number of hair per graft or still to a low hair diameter.
We also fill this way when, after a previous transplant, the contrast between the anterior hairy transplanted zone and the completely balding vertex requires to balance both areas. In that case, we just search a covering density, through more or less a thousand grafts, which also leaves the possibility of strengthening the density of the anterior zone and the midscalp.For this minimalist covering, we manage the lack. The main danger is to have an unsatisfactory pale covering. The second danger is to see, during the post-operative years, a hair recession with a halo effect developed around the transplanted zone.
It is thus recommended to increase gradually the density by starting from the center towards the periphery. (Fig 5)

Fig 5 : Minimalist covering
The purpose is to give the illusion that the center is thinning while the periphery remains dense. We can even cover only the periphery of the emptied zone without searching to cover the center of the vertex imitate perfectly a natural baldness.
For these minimalist coverings, it is highly recommended to use only small grafts, containing ideally 1 or 2 hair. Indeed, the use of richer grafts risks to give a pluggy unnatural aspect. The presence of small groups, rich in hair and separated by an important distance obviously signs the surgical origin of this aspect.
Maximum Coverage
When the patient is lucky enough to be bald only at the level of the vertex when he is over the age of 40-45 years old and when the decision to proceed to a consequent transplant is taken, the strategy is quite different.
As usual, the purpose will be to give the best possible apparent density. When we fill in the vertex with an equal density everywhere, the coverage inevitably seems to decrease when we approach the center. This is linked to the reduction of the overwhelming phenomenon which by definition is absent in the center. (The overwhelming or shingling effect is an optical effect linked to the overlapping of different hair layers.) It is a matter of realizing a set of incisions which converge to the same center while increasing gradually their density. The experience shows that it is much easier to obtain an excellent result by starting from the center towards the periphery than by trying to do the contrary. In that case, the author uses in the center a blade cut to size of dimension 0.8 to 0.9 mm for a two hair FU grafts. He squeezes as strongly as possible 50 to 100 central incisions. To use bigger transplants in the center will often give a less natural aspect. (fig 6)

Fig 6 : Maximum Coverage of the Whorl Center
Be careful however that slots don’t overlap because the consequence would be creating tears of skin on several millimeters.
Going to the periphery, we can increase the size of incisions to 1 or 1.1 mm to receive grafts of 3 or 4 hairs. Incisions are made at 1 or 2 cm from the center of the swirl in an eccentric way by respecting well the original orientation of hair. The purpose is twofold: to integrate perfectly the hair remaining in the middle of the transplanted zone but also to assure a perfect connection with the peripheral hair. To avoid the halo described here above, it is necessary to go deep into the bearing zone with obvious signs of hair loss and to blend the existing hair with the grafts. (fig 7)
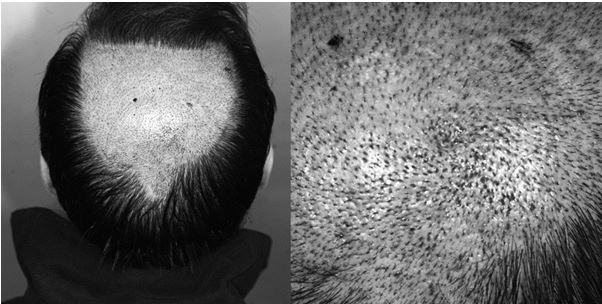
Fig 7 Maximum Covering
If we are in front of a patient whose recipient zone is relatively small and for whom we have a big quantity of grafts, it is more logical at this moment to privilege the density in the center of the vertex in order to increase the phenomenon of overwhelming from the more peripheral zones to the center. It can be made by decreasing progressively the density of the incisions from the center towards the periphery. It can also be made by privileging the use of the richest grafts at the center and the less rich in the periphery. To be noted that we are in this particular case in a completely different strategy from what has been described higher for the minimalist management.
Particular Cases
Lam (11) describes a different distribution which can be interesting to consider. The basic philosophy of his theory states that density can be achieved through two methods: by using larger sized grafts and by placing grafts closer together. Density distribution over the crown is based on a zonal priority, with zone 1 having the highest priority and zone 6 the lowest (Fig. 8). Zone 1 hair is considered the most important as it serves multiple purposes by contributing coverage to the part, midscalp and contralateral crown regions. Coverage within zone 6 is the least important because it resides in the lower aspect of the vertex and because there is no shingling effect in this area to supplement coverage over any of the neighboring vertex zones. Density priorities sequentially decrease from zone 1 to zone 6 based on the cosmetic importance and shingling contributions provided by each respective zone.

Fig 8 Lam’s Theory
Anchoring Zone
When we want the vertex to be an anchoring zone, it is also possible to distribute grafts on an important surface with a low density. These hairs will only serve to anchor the hair from the forehead and the midscalp that are combed backwards. Without support, these hairs would tend to slide on the vertex and to reveal more easily the underlying balding. Thanks to some hundreds of anchored hairs, this tendency to slide is reduced.
Exclusive Covering of the Upper Zone of the Vertex
As mentioned above, it often happens that the transplant of a crown contains not only the vertex strictly speaking but also the posterior part of the midscalp. Some authors as Unger recommend to fill in exclusively this posterior midscalp and the top of the vertex. The purpose being that a part of these grafts falls backwards and covers the untreated part of the vertex. When the vertex is completely bald, we can also change the location of the center of the swirl. He recommends a high placement to increase the quantity of hair covering the lower part of the vertex. The center of the vertex is almost always moved away from the center, most often to the right.
Results, Re-growth
Some authors noticed the fact that the grafts on the vertex tend to grow more slowly. The author has not observed this phenomenon personally.
Conclusion
Transplantation of the vertex is not easy. It requires many skills from the practitioner: a good sense of observation, a good sense of anticipation, experience, an artistic skill and a technical precision. As we have seen, there are often many strategic choices for the same situation. Each one will decide according to his experience, keeping always in mind the famous maxim : primum no nocere (first do not harm).
References
(1) Ziering C, Krenitsky G. The Ziering whorl classification of scalp
hair. Dermatol Surg 2003; 29(8): 817–21.
(2) Unger, W. Surgical Planning and Organization. In: W. Unger, R. Shapiro, R. Unger, and M. Unger, eds. Hair Transplantation, 5th edition. New York, London: Informa Healthcare, 2011, pp. 142-146.
(3) James Arnold November/December 2009 Volume 19, Number 6 page 11
(4) Norwood OT. Male pattern baldness: classification and incidence.
South Med J 1975; 68: 1359–65.
(5) Unger Unger, W.Male and female pattern hair loss. In: W. Unger, R. Shapiro, R. Unger, and M. Unger, eds. Hair Transplantation, 5th edition. New York, London: Informa Healthcare, 2011, pp. 40-42.
(6) Cohen BH. Hair loss profile, index, and severity scale. In: Haber R,
Stough D, eds. Hair Transplantation. Philadelphia: Elsevier,2006: 12.
(7). Kaufman KD, Olsen EA, Whiting D, et al. Finasteride in the
treatment of men with androgenetic alopecia. J Am Acad
Dermatol 1998; 39: 578–89.
(8). Kaufman KD: Merck Research Laboratories (The Finasteride
Male Pattern Hair Loss Study Group) Long-term (5-year)
multinational experience with finasteride 1 mg in the treatment
of men with androgenetic alopecia. Eur J Dermatol 2002; 12:
38–49.
(9) Dowling B. Stough The Paradox of Crown Transplantation International forum July/August 2005 Volume 15, Number 4
(10) Frechet P. Slot correction by a three hair-bearing transposition flap in combination with AR. Int J Aesth Rest Surg 1994; 2:27–32.
(11) Samuel M. Lam Hair transplant 360
—-
David (TakingThePlunge)
Editorial Assistant and Forum Co-Moderator for the Hair Transplant Network, the Coalition Hair Loss Learning Center, and the Hair Loss Q & A Blog.
To share ideas with other hair loss sufferers visit the hair loss forum and social community.
Technorati Tags: Hair transplantation, baldness, hair loss, alopecia, balding, male pattern baldness, bald, Propecia, finasteride, Rogaine, minoxidil, hair loss treatment, hair restoration, follicular unit, hair transplants, follicular unit extraction, FUE



September 19, 2019 @ 7:50 am
Hey Dr. Jean Devroye,
I want to thank you for providing such an article full of use information and complete study about the hair loss pattern and your research on this field.
December 11, 2014 @ 6:50 am
I must congratulate Dr Jean Devroye for a most insightful article on a difficult area in the field of surgical hair restoration.